Features
- European Union: for in vitro diagnostic use
- rest of the world: for research use only!
- incubation period 3.25 h
- antibody and enzyme conjugate: RTU
- buffer and substrate: RTU
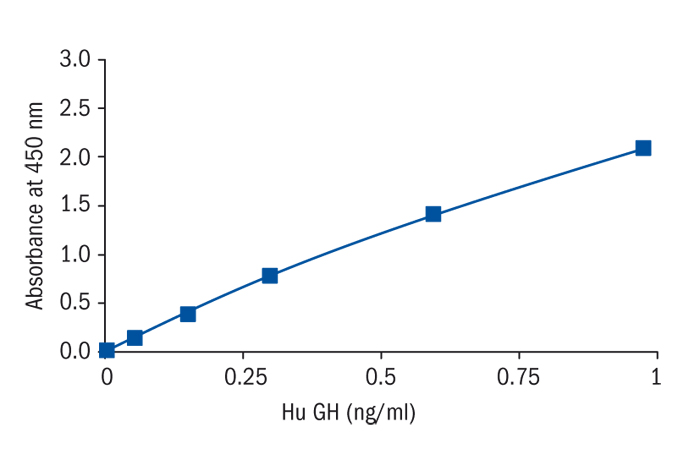
- analytical sensitivity : 0.0115 ng/ml
- assay range : 0.0115 - 26 ng/ml
- 1 control serum, freeze-dried
- intra/ interassay variance < 10%
Research topic
Growth hormone and factor-related products, Animal studies
Summary
The endocrine system of human Growth Hormone (hGH), also named Somatropin, is characterized by an extreme complexity. hGH is the product of the GH-1 gene located on chromosome 17 and expressed in pituitary cells. 80% of the gene expression results in a non-glycolsylated 22 kDa protein consisting of 191 amino acids. The other 20% of gene expression results in a variant form of 20 kDa by alternative splicing. Additionally, several more smaller variants can be found in circulation as well as translational modificated proteins and different degrees of protein aggregation. Further on, bioactivity of Growth Hormone is regulated by a specific binding protein (GHBP) formed by the extra cellular part of the cellular transmembran GH-receptor. These modifications allow a tight control of the half-life period hGH and of its bioactivity. GH is species specific.
Not only synthesis and posttranslational modification but also secretion of hGH is tightly regulated. Spontaneous pulsatile secretion takes place with a single pulse every three hours and a maximal secretion during night’s sleep. Several different attractions as physiologic stress or hypoglycaemia and amino acids result in additional hGH secretion, induced by the hypothalamic hormones Somatostatin and GH-Releasing Hormone (GHRH). Age, sexual steroids, nutritional status, illness and emotions influence the amount of secreted hGH. Because of the multitude of influencing factors the normal quantitative secretion is not known.
Physiological functions are partially exerted by Insulin-like Growth Factors (IGFs). In children and adolescent the hGH system is the main regulator of growth. If the hGH system fails totally, human growth will end at 120 cm. Beside regulation of growth hGH exerts an anabolic effect on muscle and connective tissue as wells as on bone and different other organs (heart, intestine). Further hGH was proved to have a lipolytic effect.
Growth Hormone pathology is characterized by extreme high or extreme low hGH secretion. During childhood it is the Growth Hormone deficiency congenital or acquired, which leads to microsomia. For diagnosis of Growth Hormone deficiency an hGH stimulation test has to be done or the spontaneous excretion must be investigated. The therapy consists of substitution of endogenous Growth Hormone by recombinant hGH resulting in normalization of growth.
In adulthood hGH deficiency is mostly caused by pituitary adenoma (and their surgical excision). hGH deficiency shows typical disease pattern, equivalent to advanced aging (adipositas, muscle dystrophy, arteriosclerosis, osteoporosis, adynamia). Substitutional therapy is a well-known, approved and efficient therapy of severe Growth Hormone deficiency in adulthood. Therapeutical success is directly as well as indirectly proved by measurement of IGF in serum.
Excessive hGH secretion, mostly causes by pituitary adenoma, results in childhood in gigantism, in adulthood in acromegalie, leading to enlarged extremities, diabetes, heart insufficiency and tumor growth. Surgical excision of the adenoma is the therapy of choice. If tumor excision is not possible or incomplete, a medicinal therapy with somatostatin preparation will be conducted, resulting in inhibition of hGH production. Alternatively hGH analoga (e.g. Pegvisomat) are used to block the hGH receptor and thereby inhibit action of endogenous hGH. Determination of human Growth Hormone (hGH, Somatropin) is done for diagnostic of Growth Hormone deficiency or Growth Hormone excess (arcomegaly). During medicinal and/or after surgical therapy of arcomegaly Growth Hormone (and IGF-I) measurement is used for therapy control.