Type
Recombinant protein
Description
Total 219 AA. MW: 23.9 kDa (calculated). UniProtKB acc. No. Q96CG8 (Ser31–Lys243). C-terminal His-tag (6 extra AA). Protein identity confirmed by MS.
Amino Acid Sequence
SEIPKGKQKAQLRQREVVDLYNGMCLQGPAGVPGRDGSPGANGIPGTPGIPGRDGFKGEKGECLRESFEESWTPNYKQCSWSSLNYGIDLGKIAECTFTKMRSNSALRVLFSGSLRLKCRNACCQRWYFTFNGAECSGPLPIEAIIYLDQGSPEMNSTINIHRTSSVEGLCEGIGAGLVDVAIWVGTCSDYPKGDASTGWNSVSRIIIEELPKHHHHHH
Source
HEK293
Purity
˃ 90 % by SDS-PAGE
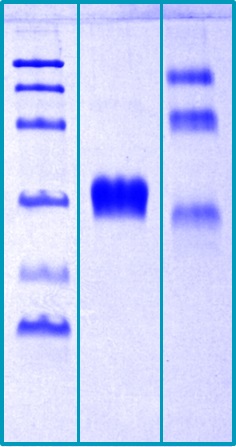
SDS-PAGE Gel
14 % SDS-PAGE separation of Human CTHRC1:
1. M.W. marker – 14, 21, 31, 45, 66, 97 kDa
2. Reduced and boiled sample, 2.5 μg/lane
3. Non-reduced and non-boiled sample, 2.5 μg/lane
Endotoxin
< 1.0 EU/µg
Formulation
Filtered (0.4 μm) and lyophilized in phosphate buffered saline pH 7.5.
Reconstitution
Add 200 µl of deionized water to prepare a working stock solution of approximately 0.5 mg/ml and let the lyophilized pellet dissolve completely.
Applications
Western blotting, ELISA
Shipping
At ambient temperature. Upon receipt, store the product at the temperature recommended below.
Storage/Expiration
Store the lyophilized protein at -80 °C. Lyophilized protein remains stable until the expiry date when stored at -80 °C. Aliquot reconstituted protein to avoid repeated freezing/thawing cycles and store at -80 °C for long term storage. Reconstituted protein can be stored at 4 °C for a week.
Quality Control Test
BCA to determine quantity of the protein.
SDS PAGE to determine purity of the protein.
Endotoxin level determination.
Note
This product is intended for research use only.
Research topic
Atherosclerosis, Bone and cartilage metabolism, Cardiovascular disease, Coronary artery disease, Energy metabolism and body weight regulation, Extracellular matrix, Oncology
Summary
Collagen triple helix repeat-containing protein 1 (CTHRC1) was identified in a screen for differentially expressed sequences in balloon-injured versus normal arteries. CTHRC1 expression was not detectable in normal arteries. However, on injury it was transiently expressed by fibroblasts of the remodeling adventitia and by smooth muscle cells of the neointima. It was also found in the matrix of calcifying human atherosclerotic plaques. CTHRC1 is a secreted 28-kDa protein that is glycosylated and highly conserved from lower chordates to mammals. A short collagen motif with 12 Gly-X-Y repeats appears to be responsible for trimerization of the protein and this renders the molecule susceptible to cleavage by collagenase. CTHRC1 is highly associated with calcified tissues and cartilaginous matrix, but not with endothelial cells. This is consistent with expression study results that showed CTHRC1 to be highly expressed in the developing skull bones, ribs, vertebrae, and cartilage primordia. CTHRC1 is a circulating factor detectable qualitatively in plasma of healthy human subjects. CTHRC1 plasma levels were also significantly elevated during pregnancy, in diabetes, in inflammatory and infectious conditions, in subjects with acute myeloid leukemia but not in subjects with solid cancers. Hormonal functions of CTHRC1 include regulation of lipid storage and cellular glycogen levels with potentially broad implications for cell metabolism and physiology. Deletion of the CTHRC1 gene leads to fatty liver (steatosis) formation in mice while others showed that inactivation of this gene also results in low bone mass. CTHRC1 was identified in skeletal and cardiac muscles of mice, representing Duchenne and congenital muscle dystrophies (DMD and CMD) and dysferlinopathy. CTHRC1 is involved in postnatal bone formation and is secreted by mature functional osteoclasts. It acts on stromal/osteoblastic cells by binding to a putative cell surface receptor in order to stimulate osteoblastic differentiation as well as recruitment, thereby promoting bone formation. Among the cancer cells reported to express CTHRC1 are melanomas, hepatocellular carcinoma, oral cancer, breast ductal carcinoma, pancreatic cancer, colorectal cancer, gastric cancer, and dermatofibrosarcoma protuberans, but a more recent study demonstrated that CTHRC1 expression in human cancers originates from activated stromal cells, not from the tumor cells themselves. CTHRC1 may have therapeutic value in antifibrotic treatment strategies and could have major clinical applications in the fields of vascular disease, repair, and fibrosis. The results indicate that CTHRC1 increases bone mass as a positive regulator of osteoblastic bone formation and offers an anabolic approach for the treatment of osteoporosis. CTHRC1 could serve as a potential marker for predicting progression and metastasis of the aforementioned types of cancers.