Type
Sandwich ELISA, HRP-labelled antibody
Description
The RIS006R Human Insulin ELISA Immunoenzymetric assay for the measurement of human Insulin in serum.
Applications
Serum
Sample Requirements
50 µl/well
Shipping
On blue ice packs. Upon receipt, store the product at the temperature recommended below.
Storage/Expiration
Store the complete kit at 2–8°C. Under these conditions, the kit is stable until the expiration date (see label on the box).
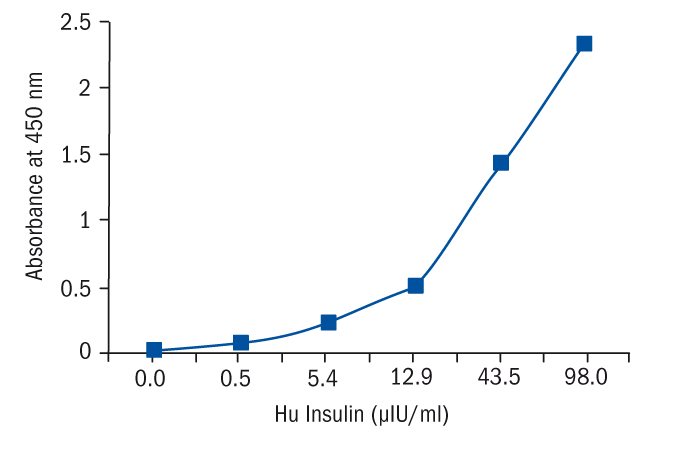
Calibration Curve
Calibration Range
5.1–250 µIU/ml
Limit of Detection
0.17 µIU/ml
Intra-assay (Within-Run)
CV < 10%
Inter-assay (Run-to-Run)
CV < 10%
Features
- RUO
- calibration range 5.1–250 µIU/ml
- limit of detection 0.17 µIU/ml
- quality controls
Research topic
Diabetology - Insulin, C-Peptide, Proinsulin, Energy metabolism and body weight regulation
Summary
Biological activities of insulin:
Insulin, a polypeptide hormone with a molecular weight of 5800 Da, is secreted by the beta cells of the islets of Langerhans from the pancreas. Insulin possesses a wide spectrum of biological actions. It stimulates cellular glucose uptake, glucose oxidation, glycogenesis, lipogenesis, proteogenesis and the formation of DNA and RNA. Insulin plays a key role in the regulation of plasma glucose levels (hepatic output inhibition, stimulation of peripheral glucose utilisation). The resulting hypoglycemic effects of insulin are counterbalanced by hormones with hyperglycemic effects (glucagon, growth hormone, cortisol, epinephrin). Insulin secretion is mainly controlled by the plasma glucose levels : hyperglycemia induces a prompt and important increase in circulating insulin levels. Neural influences, as well as various metabolic and hormonal factors (amino acids, glucagon, gastro intestinal hormone) also participate to the control of insulin secretion. Type I (insulin dependent : "juvenile") diabetes is due to a destruction of the beta cells, with a consequence of absolute lack of insulin. In type II (non-insulin-dependent : "maturity onset") diabetes, insulin resistance may play an important role; however after several years of evolution, beta-cells failure may occur, leading to a relative insulinopenia requiring, in some cases, insulin administration. Insulin resistance is associated with high circulation levels of the hormone.
The most common case of insulin resistance is represented by obesity.
Various endocrinopathies (acromegaly, Cushing syndrome) as well as rare cases of insulin receptor defects or cases with anti-insulin receptor antibodies are associated with glucose intolerance or even diabetes due to insulin resistance. The determination of plasma insulin levels is an important parameter in the diagnosis of hypoglycemia. Insulin levels are high in cases of insulinoma (beta-cell tumor). Functional postprandial hypoglycemia may also be associated with inappropriate insulin release to carbohydrate intake. Insulin levels are determined either in the fasting state or during dynamic test:
a) stimulation test : carbohydrate rich meal, oral glucose tolerance test (OGTT), arginin infusion, tolbutamide or other sulfonylureas administration.
b) inhibition test : fasting, somatostatine infusion
Clinical application of insulin determination:
Determination of the beta-cell reserve during glucose tolerance test or after a carbohydrate rich meal, as a guide for the instauration of insulin therapy;
Contribution to the diagnosis of insulin and non-insulin-dependent diabetes;
Characterisation and follow-up of states of glucose intolerance;
Diagnosis and study of cases of insulin resistance;
Diagnosis of insulinoma and other causes of hypoglycemia.
Find documents for the lot
Example Instructions for Use (RUO)
Example Instructions for Use (RUO)
Safety Information (RUO)
MSDS (RUO)